4. The Fasciæ and Muscles of the Head. a. The Muscles of the Scalp
Epicranius
The Skin of the Scalp.—This is thicker than in any other part of the body. It is intimately adherent to the superficial fascia, which attaches it firmly to the underlying aponeurosis and muscle. Movements of the muscle move the skin. The hair follicles are very closely set together, and extend throughout the whole thickness of the skin. It also contains a number of sebaceous glands.
The superficial fascia in the cranial region is a firm, dense, fibro-fatty layer, intimately adherent to the integument, and to the Epicranius and its tendinous aponeurosis; it is continuous, behind, with the superficial fascia at the back of the neck; and, laterally, is continued over the temporal fascia. It contains between its layers the superficial vessels and nerves and much granular fat.
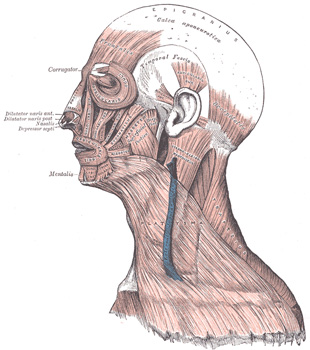
The Epicranius (Occipitofrontalis) (Fig. 378) is a broad, musculofibrous layer, which covers the whole of one side of the vertex of the skull, from the occipital bone to the eyebrow. It consists of two parts, the Occipitalis and the Frontalis, connected by an intervening tendinous aponeurosis, the galea aponeurotica.
The Occipitalis, thin and quadrilateral in form, arises by tendinous fibers from the lateral two-thirds of the superior nuchal line of the occipital bone, and from the mastoid part of the temporal. It ends in the galea aponeurotica.
The Frontalis is thin, of a quadrilateral form, and intimately adherent to the superficial fascia. It is broader than the Occipitalis and its fibers are longer and paler in color. It has no bony attachments. Its medial fibers are continuous with those of the Procerus; its immediate fibers blend with the Corrugator and Orbicularis oculi; and its lateral fibers are also blended with the latter muscle over the zygomatic process of the frontal bone. From these attachments the fibers are directed upward, and join the galea aponeurotica below the coronal suture. The medial margins of the Frontales are joined together for some distance above the root of the nose; but between the Occipitales there is a considerable, though variable, interval, occupied by the galea aponeurotica.
The galea aponeurotica (epicranial aponeurosis) covers the upper part of the cranium; behind, it is attached, in the interval between its union with the Occipitales, to the external occipital protuberance and highest nuchal lines of the occipital bone; in front, it forms a short and narrow prolongation between its union with the Frontales. On either side it gives origin to the Auriculares anterior and superior; in this situation it loses its aponeurotic character, and is continued over the temporal fascia to the zygomatic arch as a layer of laminated areolar tissue. It is closely connected to the integument by the firm, dense, fibro-fatty layer which forms the superficial fascia of the scalp: it is attached to the pericranium by loose cellular tissue, which allows the aponeurosis, carrying with it the integument to move through a considerable distance.
Variations.—Both Frontalis and Occipitalis vary considerably in size and in extent of attachment; either may be absent; fusion of Frontalis to skin has been noted.
Nerves.—The Frontalis is supplied by the temporal branches of the facial nerve, and the Occipitalis by the posterior auricular branch of the same nerve.
Actions.—The Frontales raise the eyebrows and the skin over the root of the nose, and at the same time draw the scalp forward, throwing the integument of the forehead into transverse wrinkles. The Occipitales draw the scalp backward. By bringing alternately into action the Frontales and Occipitales the entire scalp may be moved forward and backward. In the ordinary action of the muscles, the eyebrows are elevated, and at the same time the aponeurosis is fixed by the Occipitales, thus giving to the face the expression of surprise; if the action be exaggerated, the eyebrows are still further raised, and the skin of the forehead thrown into transverse wrinkles, as in the expression of fright or horror.
A thin muscular slip, the Transversus nuchæ, is present in a considerable proportion (25 per cent.) of cases; it arises from the external occipital protuberance or from the superior nuchal line, either superficial or deep to the Trapezius; it is frequently inserted with the Auricularis posterior, but may join the posterior edge of the Sternocleidomastoideus.
The United States Medical Licensing Examination (USMLE) is a three-step examination for medical licensure in the United States. The Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME) sponsors USMLE.
The Three Steps of the USMLE
Step 1 tests the important concepts of basic sciences basic to the practice of medicine. It also places special emphasis on principles and mechanisms underlying health, disease, and modes of therapy. Step 1 ensures mastery of the sciences that provide a foundation for the safe and competent practice of medicine. It also tests the scientific principles required for maintenance of competence through lifelong learning.
Step 2 CK tests the medical knowledge, skills, and understanding of clinical science essential for the provision of patient care under supervision. It also includes emphasis on health promotion and disease prevention. Step 2 CK ensures that due attention is devoted to principles of clinical sciences and basic patient-centered skills.
Step 2 CS tests your capacity to practice and provide good medical service in real-life situations. It also tests your communication skills.
Step 3 tests your medical knowledge and understanding of biomedical and clinical science essential for the unsupervised practice of medicine. Step 3 provides a final assessment of physicians assuming independent responsibility for delivering general medical care.