The thoracic vertebræ(Fig. 90) are intermediate in size between those of the cervical and lumbar regions; they increase in size from above downward, the upper vertebræ being much smaller than those in the lower part of the region. They are distinguished by the presence of facets on the sides of the bodies for articulation with the heads of the ribs, and facets on the transverse processes of all, except the eleventh and twelfth, for articulation with the tubercles of the ribs.
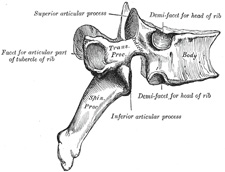
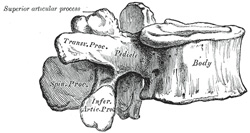
The bodies in the middle of the thoracic region are heart-shaped, and as broad in the antero-posterior as in the transverse direction. At the ends of the thoracic region they resemble respectively those of the cervical and lumbar vertebræ. They are slightly thicker behind than in front, flat above and below, convex from side to side in front, deeply concave behind, and slightly constricted laterally and in front. They present, on either side, two costal demi-facets, one above, near the root of the pedicle, the other below, in front of the inferior vertebral notch; these are covered with cartilage in the fresh state, and, when the vertebræ are articulated with one another, form, with the intervening intervertebral fibrocartilages, oval surfaces for the reception of the heads of the ribs. The pedicles are directed backward and slightly upward, and the inferior vertebral notches are of large size, and deeper than in any other region of the vertebral column. The laminæ are broad, thick, and imbricated—that is to say, they overlap those of subjacent vertebræ like tiles on a roof. The vertebral foramen is small, and of a circular form. The spinous process is long, triangular on coronal section, directed obliquely downward, and ends in a tuberculated extremity. These processes overlap from the fifth to the eighth, but are less oblique in direction above and below. The superior articular processes are thin plates of bone projecting upward from the junctions of the pedicles and laminæ; their articular facets are practically flat, and are directed backward and a little lateralward and upward. The inferior articular processes are fused to a considerable extent with the laminæ, and project but slightly beyond their lower borders; their facets are directed forward and a little medialward and downward. The transverse processes arise from the arch behind the superior articular processes and pedicles; they are thick, strong, and of considerable length, directed obliquely backward and lateralward, and each ends in a clubbed extremity, on the front of which is a small, concave surface, for articulation with the tubercle of a rib. The first, ninth, tenth, eleventh, and twelfth thoracic vertebræ present certain peculiarities, and must be specially considered (Fig. 91).
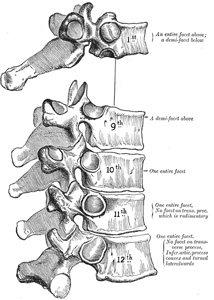
The First Thoracic Vertebra has, on either side of the body, an entire articular facet for the head of the first rib, and a demi-facet for the upper half of the head of the second rib. The body is like that of a cervical vertebra, being broad transversely; its upper surface is concave, and lipped on either side. The superior articular surfaces are directed upward and backward; the spinous process is thick, long, and almost horizontal. The transverse processes are long, and the upper vertebral notches are deeper than those of the other thoracic vertebræ.
The Ninth Thoracic Vertebra may have no demi-facets below. In some subjects however, it has two demi-facets on either side; when this occurs the tenth has only demi-facets at the upper part.
The Tenth Thoracic Vertebra has (except in the cases just mentioned) an entire articular facet on either side, which is placed partly on the lateral surface of the pedicle.
In the Eleventh Thoracic Vertebra the body approaches in its form and size to that of the lumbar vertebræ. The articular facets for the heads of the ribs are of large size, and placed chiefly on the pedicles, which are thicker and stronger in this and the next vertebra than in any other part of the thoracic region. The spinous process is short, and nearly horizontal in direction. The transverse processes are very short, tuberculated at their extremities, and have no articular facets.
The Twelfth Thoracic Vertebra has the same general characteristics as the eleventh, but may be distinguished from it by its inferior articular surfaces being convex and directed lateralward, like those of the lumbar vertebræ; by the general form of the body, laminæ, and spinous process, in which it resembles the lumbar vertebræ; and by each transverse process being subdivided into three elevations, the superior, inferior, and lateral tubercles: the superior and inferior correspond to the mammillary and accessory processes of the lumbar vertebræ. Traces of similar elevations are found on the transverse processes of the tenth and eleventh thoracic vertebræ.
The United States Medical Licensing Examination (USMLE) is a three-step examination for medical licensure in the United States. The Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME) sponsors USMLE.
The Three Steps of the USMLE
Step 1 tests the important concepts of basic sciences basic to the practice of medicine. It also places special emphasis on principles and mechanisms underlying health, disease, and modes of therapy. Step 1 ensures mastery of the sciences that provide a foundation for the safe and competent practice of medicine. It also tests the scientific principles required for maintenance of competence through lifelong learning.
Step 2 CK tests the medical knowledge, skills, and understanding of clinical science essential for the provision of patient care under supervision. It also includes emphasis on health promotion and disease prevention. Step 2 CK ensures that due attention is devoted to principles of clinical sciences and basic patient-centered skills.
Step 2 CS tests your capacity to practice and provide good medical service in real-life situations. It also tests your communication skills.
Step 3 tests your medical knowledge and understanding of biomedical and clinical science essential for the unsupervised practice of medicine. Step 3 provides a final assessment of physicians assuming independent responsibility for delivering general medical care.