The sternoclavicular articulation is a double arthrodial joint. The parts entering into its formation are the sternal end of the clavicle, the upper and lateral part of the manubrium sterni, and the cartilage of the first rib. The articular surface of the clavicle is much larger than that of the sternum, and is invested with a layer of cartilage, 68 which is considerably thicker than that on the latter bone. The ligaments of this joint are:
The Articular Capsule (capsula articularis; capsular ligament).—The articular capsule surrounds the articulation and varies in thickness and strength. In front and behind it is of considerable thickness, and forms the anterior and posterior sternoclavicular ligaments; but above, and especially below, it is thin and partakes more of the character of areolar than of true fibrous tissue.
The Anterior Sternoclavicular Ligament (ligamentum sternoclaviculare anterior).—The anterior sternoclavicular ligament is a broad band of fibers, covering the anterior surface of the articulation; it is attached above to the upper and front part of the sternal end of the clavicle, and, passing obliquely downward and medialward, is attached below to the front of the upper part of the manubrium sterni. This ligament is covered by the sternal portion of the Sternocleidomastoideus and the integument; behind, it is in relation with the capsule, the articular disk, and the two synovial membranes.
The Posterior Sternoclavicular Ligament (ligamentum sternoclaviculare posterius).—The posterior sternoclavicular ligament is a similar band of fibers, covering the posterior surface of the articulation; it is attached above to the upper and back part of the sternal end of the clavicle, and, passing obliquely downward and medialward, is fixed below to the back of the upper part of the manubrium sterni. It is in relation, in front, with the articular disk and synovial membranes; behind, with the Sternohyoideus and Sternothyreoideus.
The Interclavicular Ligament (ligamentum interclaviculare).—This ligament is a flattened band, which varies considerably in form and size in different individuals, it passes in a curved direction from the upper part of the sternal end of one clavicle to that of the other, and is also attached to the upper margin of the sternum. It is in relation, in front, with the integument and Sternocleidomastoidei; behind, with the Sternothyreoidei.
The Costoclavicular Ligament (ligamentum costoclaviculare; rhomboid ligament).—This ligament is short, flat, strong, and rhomboid in form. Attached below to the upper and medial part of the cartilage of the first rib, it ascends obliquely backward and lateralward, and is fixed above to the costal tuberosity on the under surface of the clavicle. It is in relation, in front, with the tendon of origin of the Subclavius; behind, with the subclavian vein.
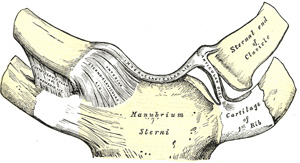
FIG. 325– Sternoclavicular articulation. Anterior view. (See enlarged image)
The Articular Disk (discus articularis).—The articular disk is flat and nearly circular, interposed between the articulating surfaces of the sternum and clavicle. It is attached, above, to the upper and posterior border of the articular surface of the clavicle; below, to the cartilage of the first rib, near its junction with the sternum; and by its circumference to the interclavicular and anterior and posterior sternoclavicular ligaments. It is thicker at the circumference, especially its upper and back part, than at its center. It divides the joint into two cavities, each of which is furnished with a synovial membrane.
Synovial Membranes.—Of the two synovial membranes found in this articulation, the lateral is reflected from the sternal end of the clavicle, over the adjacent surface of the articular disk, and around the margin of the facet on the cartilage of the first rib; the medial is attached to the margin of the articular surface of the sternum and clothes the adjacent surface of the articular disk; the latter is the larger of the two.
Movements.—This articulation admits of a limited amount of motion in nearly every direction—upward, downward, backward, forward, as well as circumduction. When these movements take place in the joint, the clavicle in its motion carries the scapula with it, this bone gliding on the outer surface of the chest. This joint therefore forms the center from which all movements of the supporting arch of the shoulder originate, and is the only point of articulation of the shoulder girdle with the trunk. The movements attendant on elevation and depression of the shoulder take place between the clavicle and the articular disk, the bone rotating upon the ligament on an axis drawn from before backward through its own articular facet; when the shoulder is moved forward and backward, the clavicle, with the articular disk rolls to and fro on the articular surface of the sternum, revolving, with a sliding movement, around an axis drawn nearly vertically through the sternum; in the circumduction of the shoulder, which is compounded of these two movements, the clavicle revolves upon the articular disk and the latter, with the clavicle, rolls upon the sternum. 69 Elevation of the shoulder is limited principally by the costoclavicular ligament; depression, by the interclavicular ligament and articular disk. The muscles which raise the shoulder are the upper fibers of the Trapezius, the Levator scapulæ, and the clavicular head of the Sternocleidomastoideus, assisted to a certain extent by the Rhomboidei, which pull the vertebral border of the scapula backward and upward and so raise the shoulder. The depression of the shoulder is principally effected by gravity assisted by the Subclavius, Pectoralis minor and lower fibers of the Trapezius. The shoulder is drawn backward by the Rhomboidei and the middle and lower fibers of the Trapezius, and forward by the Serratus anterior and Pectoralis minor.
The United States Medical Licensing Examination (USMLE) is a three-step examination for medical licensure in the United States. The Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME) sponsors USMLE.
The Three Steps of the USMLE
Step 1 tests the important concepts of basic sciences basic to the practice of medicine. It also places special emphasis on principles and mechanisms underlying health, disease, and modes of therapy. Step 1 ensures mastery of the sciences that provide a foundation for the safe and competent practice of medicine. It also tests the scientific principles required for maintenance of competence through lifelong learning.
Step 2 CK tests the medical knowledge, skills, and understanding of clinical science essential for the provision of patient care under supervision. It also includes emphasis on health promotion and disease prevention. Step 2 CK ensures that due attention is devoted to principles of clinical sciences and basic patient-centered skills.
Step 2 CS tests your capacity to practice and provide good medical service in real-life situations. It also tests your communication skills.
Step 3 tests your medical knowledge and understanding of biomedical and clinical science essential for the unsupervised practice of medicine. Step 3 provides a final assessment of physicians assuming independent responsibility for delivering general medical care.