5g. Articulation of the Manubrium and Body of the Sternum
The manubrium is united to the body of the sternum either by an amphiarthrodial joint—a piece of fibrocartilage connecting the segments—or by a diarthrodial joint, in which the articular surface of each bone is clothed with a lamina of cartilage. In the latter case, the cartilage covering the body is continued without interruption on to the cartilages of the facets for the second ribs. Rivington found the diarthrodial form of joint in about one-third of the specimens examined by him, Maisonneuve more frequently. It appears to be rare in childhood, and is formed, in Rivington’s opinion, from the amphiarthrodial form, by absorption. The diarthrodial joint seems to have no tendency to ossify, while the amphiarthrodial is more liable to do so, and has been found ossified as early as thirty-four years of age. The two segments are further connected by anterior and posterior intersternal ligaments consisting of longitudinal fibers.
Mechanism of the Thorax.—Each rib possesses its own range and variety of movements, but the movements of all are combined in the respiratory excursions of the thorax. Each rib may be regarded as a lever the fulcrum of which is situated immediately outside the costotransverse articulation, so that when the body of the rib is elevated the neck is depressed and vice versa; from the disproportion in length of the arms of the lever a slight movement at the vertebral end of the rib is greatly magnified at the anterior extremity.
The anterior ends of the ribs lie on a lower plane than the posterior; when therefore the body of the rib is elevated the anterior extremity is thrust also forward. Again, the middle of the body of the rib lies in a plane below that passing through the two extremities, so that when the body is elevated relatively to its ends it is at the same time carried outward from the median plane of the thorax. Further, each rib forms the segment of a curve which is greater than that of the rib immediately above, and therefore the elevation of a rib increases the transverse diameter of the thorax in the plane to which it is raised. The modifications of the rib movements at their vertebral ends have already been described (page 302). Further modifications result from the attachments of their anterior extremities, and it is convenient therefore to consider separately the movements of the ribs of the three groups—vertebrosternal, vertebrochondral, and vertebral.
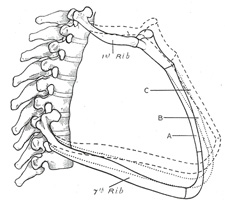
FIG. 316– Lateral view of first and seventh ribs in position, showing the movements of the sternum and ribs in A, ordinary expiration; B, quiet inspiration; C, deep inspiration. (See enlarged image)
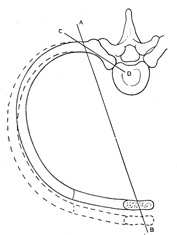
FIG. 317– Diagram showing the axes of movement (A B and C D) of a vertebrosternal rib. The interrupted lines indicate the position of the rib in inspiration. (See enlarged image)
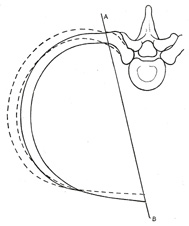
FIG. 318– Diagram showing the axis of movement (A B) of a vertebrochondral rib. The interrupted lines indicate the position of the rib in inspiration. (See enlarged image)
Vertebrosternal Ribs (Figs. 316, 317).—The first rib differs from the others of this group in that its attachment to the sternum is a rigid one; this is counterbalanced to some extent by the fact that its head possesses no interarticular ligament, and is therefore more movable. The first pair of ribs with the manubrium sterni move as a single piece, the anterior portion being elevated by rotatory movements at the vertebral extremities. In normal quiet respiration the movement of this arc is practically nil; when it does occur the anterior part is raised and carried forward, increasing the antero-posterior and transverse diameters of this region of the chest. The movement of the second rib is also slight in normal respiration, as its anterior extremity is fixed to the manubrium, and prevented therefore from moving upward. The sternocostal articulation, however, allows the middle of the body of the rib to be drawn up, and in this way the transverse thoracic diameter is increased. Elevation of the third, fourth, fifth, and sixth ribs raises and thrusts forward their anterior extremities, the greater part of the movement being effected by the rotation of the rib neck backward. The thrust of the anterior extremities carries forward and upward the body of the sternum, which moves on the joint between it and the manubrium, and thus the antero-posterior thoracic diameter is increased. This movement is, however, soon arrested, and the elevating force is then expended in raising the middle part of the body of the rib and everting its lower border; at the same time the costochondral angle is opened out. By these latter movements a considerable increase in the transverse diameter of the thorax is effected.
Vertebrochondral Ribs (Fig. 318).—The seventh rib is included with this group, as it conforms more closely to their type. While the movements of these ribs assist in enlarging the thorax for respiratory purposes, they are also concerned in increasing the upper abdominal space for viscera displaced by the action of the diaphragm. The costal cartilages articulate with one another, so that each pushes up that above it, the final thrust being directed to pushing forward and upward the lower end of the body of the sternum. The amount of elevation of the anterior extremities is limited on account of the very slight rotation of the rib neck. Elevation of the shaft is accompanied by an outward and backward movement; the outward movement everts the anterior end of the rib and opens up the subcostal angle, while the backward movement pulls back the anterior extremity and counteracts the forward thrust due to its elevation; this latter is most noticeable in the lower ribs, which are the shortest. The total result is a considerable increase in the transverse and a diminution in the median antero-posterior diameter of the upper part of the abdomen; at the same time, however, the lateral antero-posterior diameters of the abdomen are increased.
Vertebral Ribs.—Since these ribs have free anterior extremities and only costocentral articulations with no interarticular ligaments, they are capable of slight movements in all directions. When the other ribs are elevated these are depressed and fixed to form points of action for the diaphragm.
The United States Medical Licensing Examination (USMLE) is a three-step examination for medical licensure in the United States. The Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME) sponsors USMLE.
The Three Steps of the USMLE
Step 1 tests the important concepts of basic sciences basic to the practice of medicine. It also places special emphasis on principles and mechanisms underlying health, disease, and modes of therapy. Step 1 ensures mastery of the sciences that provide a foundation for the safe and competent practice of medicine. It also tests the scientific principles required for maintenance of competence through lifelong learning.
Step 2 CK tests the medical knowledge, skills, and understanding of clinical science essential for the provision of patient care under supervision. It also includes emphasis on health promotion and disease prevention. Step 2 CK ensures that due attention is devoted to principles of clinical sciences and basic patient-centered skills.
Step 2 CS tests your capacity to practice and provide good medical service in real-life situations. It also tests your communication skills.
Step 3 tests your medical knowledge and understanding of biomedical and clinical science essential for the unsupervised practice of medicine. Step 3 provides a final assessment of physicians assuming independent responsibility for delivering general medical care.