This is a ginglymo-arthrodial joint; the parts entering into its formation on either side are: the anterior part of the mandibular fossa of the temporal bone and the articular tubercle above; and the condyle of the mandible below. The ligaments of the joint are the following:
The Articular Capsule (capsula articularis; capsular ligament).—The articular capsule is a thin, loose envelope, attached above to the circumference of the mandibular fossa and the articular tubercle immediately in front; below, to the neck of the condyle of the mandible.
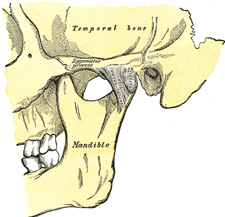
FIG. 309– Articulation of the mandible. Lateral aspect. (See enlarged image)
The Temporomandibular Ligament (ligamentum temporomandibulare; external lateral ligament) (Fig. 309).—The temporomandibular ligament consists of two short, narrow fasciculi, one in front of the other, attached, above, to the lateral surface of the zygomatic arch and to the tubercle on its lower border; below, to the lateral surface and posterior border of the neck of the mandible. It is broader above than below, and its fibers are directed obliquely downward and backward. It is covered by the parotid gland, and by the integument.
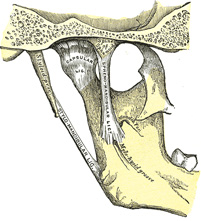
The Sphenomandibular Ligament (ligamentum sphenomandibulare; internal lateral ligament) (Fig. 310).—The sphenomandibular ligament is a flat, thin band which is attached above to the spina angularis of the sphenoid bone, and, becoming broader as it descends, is fixed to the lingula of the mandibular foramen. Its lateral surface is in relation, above, with the Pterygoideus externus; lower down, it is separated from the neck of the condyle by the internal maxillary vessels; still lower, the inferior alveolar vessels and nerve and a lobule of the parotid gland lie between it and the ramus of the mandible. Its medial surface is in relation with the Pterygoideus internus.
The Articular Disk (discus articularis; interarticular fibrocartilage; articular meniscus) (Fig. 311).—The articular disk is a thin, oval plate, placed between the condyle of the mandible and the mandibular fossa. Its upper surface is concavo-convex from before backward, to accommodate itself to the form of the mandibular fossa and the articular tubercle. Its under surface, in contact with the condyle, is concave. Its circumference is connected to the articular capsule; and in front to the tendon of the Pterygoideus externus. It is thicker at its periphery, especially behind, than at its center. The fibers of which it is composed have a concentric arrangement, more apparent at the circumference than at the center. It divides the joint into two cavities, each of which is furnished with a synovial membrane.
FIG. 310– Articulation of the mandible. Medial aspect. (See enlarged image)
FIG. 311– Sagittal section of the articulation of the mandible. (See enlarged image)
The Synovial Membranes.—The synovial membranes, two in number, are placed one above, and the other below, the articular disk. The upper one, the larger and looser of the two, is continued from the margin of the cartilage covering the mandibular fossa and articular tubercle on to the upper surface of the disk. The lower one passes from the under surface of the disk to the neck of the condyle, being prolonged a little farther downward behind than in front. The articular disk is sometimes perforated in its center, and the two cavities then communicate with each other.
The Stylomandibular Ligament (ligamentum stylomandibulare); stylomaxillary ligament(Fig. 310).—The stylomandibular ligament is a specialized band of the cervical fascia, which extends from near the apex of the styloid process of the temporal bone to the angle and posterior border of the ramus of the mandible, between the Masseter and Pterygoideus internus. This ligament separates the parotid from the submaxillary gland, and from its deep surface some fibers of the Styloglossus take origin. Although classed among the ligaments of the temporomandibular joint, it can only be considered as accessory to it.
The nerves of the temporomandibular joint are derived from the auriculotemporal and masseteric branches of the mandibular nerve, the arteries from the superficial temporal branch of the external carotid.
Movements.—The movements permitted in this articulation are extensive. Thus, the mandible may be depressed or elevated, or carried forward or backward; a slight amount of side-to-side movement is also permitted. It must be borne in mind that there are two distinct joints in this articulation—one between the condyle and the articular disk, and another between the disk and the mandibular fossa. When the mouth is but slightly opened, as during ordinary conversation, the movement is confined to the lower of the two joints. On the other hand, when the mouth is opened more widely, both joints are concerned in the movement; in the lower joint the movement is of a hinge-like character, the condyle moving around a transverse axis on the disk, while in the upper joint the movement is of a gliding character, the disk, together with the condyle, gliding forward on to the articular tubercle, around an axis which passes through the mandibular foramina. These two movements take place simultaneously, the condyle and disk move forward on the eminence, and at the same time the condyle revolves on the disk. In shutting the mouth the reverse action takes place; the disk glides back, carrying the condyle with it, and this at the same time moves back to its former position. When the mandible is carried horizontally forward, as in protruding the lower incisor teeth in front of the upper, the movement takes place principally in the upper joint, the disk and the condyle gliding forward on the mandibular fossa and articular tubercle. The grinding or chewing movement is produced by one condyle, with its disk, gliding alternately forward and backward, while the other condyle moves simultaneously in the opposite direction; at the same time the condyle undergoes a vertical rotation on the disk. One condyle advances and rotates, the other condyle recedes and rotates, in alternate succession.
The mandible is depressed by its own weight, assisted by the Platysma, the Digastricus, the Mylohyoideus, and the Geniohyoideus. It is elevated by the Masseter, Pterygoideus internus, and the anterior part of the Temporalis. It is drawn forward by the simultaneous action of the Pterygoidei internus and externus, the superficial fibers of the Masseter and the anterior fibers of the Temporalis; and backward by the deep fibers of the Masseter and the posterior fibers of the Temporalis. The grinding movement is caused by the alternate action of the Pterygoidei of either side.
The United States Medical Licensing Examination (USMLE) is a three-step examination for medical licensure in the United States. The Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME) sponsors USMLE.
The Three Steps of the USMLE
Step 1 tests the important concepts of basic sciences basic to the practice of medicine. It also places special emphasis on principles and mechanisms underlying health, disease, and modes of therapy. Step 1 ensures mastery of the sciences that provide a foundation for the safe and competent practice of medicine. It also tests the scientific principles required for maintenance of competence through lifelong learning.
Step 2 CK tests the medical knowledge, skills, and understanding of clinical science essential for the provision of patient care under supervision. It also includes emphasis on health promotion and disease prevention. Step 2 CK ensures that due attention is devoted to principles of clinical sciences and basic patient-centered skills.
Step 2 CS tests your capacity to practice and provide good medical service in real-life situations. It also tests your communication skills.
Step 3 tests your medical knowledge and understanding of biomedical and clinical science essential for the unsupervised practice of medicine. Step 3 provides a final assessment of physicians assuming independent responsibility for delivering general medical care.