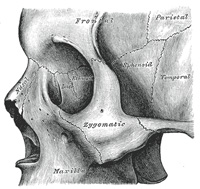
The zygomatic bone is small and quadrangular, and is situated at the upper and lateral part of the face: it forms the prominence of the cheek, part of the lateral wall and floor of the orbit, and parts of the temporal and infratemporal fossæ (Fig. 164). It presents a malar and a temporal surface; four processes, the frontosphenoidal, orbital, maxillary, and temporal; and four borders.
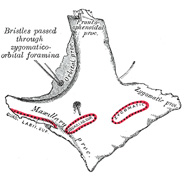
Surfaces.—The malar surface(Fig. 165) is convex and perforated near its center by a small aperture, the zygomaticofacial foramen, for the passage of the zygomaticofacial nerve and vessels; below this foramen is a slight elevation, which gives origin to the Zygomaticus.
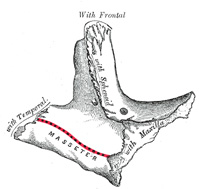
The temporal surface(Fig. 166), directed backward and medialward, is concave, presenting medially a rough, triangular area, for articulation with the maxilla, and laterally a smooth, concave surface, the upper part of which forms the anterior boundary of the temporal fossa, the lower a part of the infratemporal fossa. Near the center of this surface is the zygomaticotemporal foramen for the transmission of the zygomaticotemporal nerve.
Processes.—The frontosphenoidal process is thick and serrated, and articulates with the zygomatic process of the frontal bone. On its orbital surface, just within the orbital margin and about 11 mm. below the zygomaticofrontal suture is a tubercle of varying size and form, but present in 95 per cent. of skulls (Whitnall43). The orbital process is a thick, strong plate, projecting backward and medialward from the orbital margin. Its antero-medial surface forms, by its junction with the orbital surface of the maxilla and with the great wing of the sphenoid, part of the floor and lateral wall of the orbit. On it are seen the orifices of two canals, the zygomaticoörbital foramina; one of these canals opens into the temporal fossa, the other on the malar surface of the bone; the former transmits the zygomaticotemporal, the latter the zygomaticofacial nerve. Its postero-lateral surface, smooth and convex, forms parts of the temporal and infratemporal fossæ. Its anterior margin, smooth and rounded, is part of the circumference of the orbit. Its superiormargin, rough, and directed horizontally, articulates with the frontal bone behind the zygomatic process. Its posterior margin is serrated for articulation, with the great wing of the sphenoid and the orbital surface of the maxilla. At the angle of junction of the sphenoidal and maxillary portions, a short, concave, non-articular part is generally seen; this forms the anterior boundary of the inferior orbital fissure: occasionally, this non-articular part is absent, the fissure then being completed by the junction of the maxilla and sphenoid, or by the interposition of a small sutural bone in the angular interval between them. The maxillary process presents a rough, triangular surface which articulates with the maxilla. The temporal process, long, narrow, and serrated, articulates with the zygomatic process of the temporal.
Borders.—The antero-superior or orbital border is smooth, concave, and forms a considerable part of the circumference of the orbit. The antero-inferior or maxillary border is rough, and bevelled at the expense of its inner table, to articulate with the maxilla; near the orbital margin it gives origin to the Quadratus labii superioris. The postero-superior or temporal border, curved like an italic letter f, is continuous above with the commencement of the temporal line, and below with the upper border of the zygomatic arch; the temporal fascia is attached to it. The postero-inferior or zygomatic border affords attachment by its rough edge to the Masseter.
—The zygomatic bone is generally described as ossifying from three centers—one for the malar and two for the orbital portion; these appear about the eighth week and fuse about the fifth month of fetal life. Mall describes it as being ossified from one center which appears just beneath and to the lateral side of the orbit. After birth, the bone is sometimes divided by a horizontal suture into an upper larger, and a lower smaller division. In some quadrumana the zygomatic bone consists of two parts, an orbital and a malar.
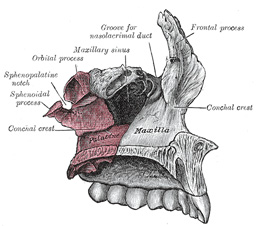
FIG. 167– Articulation of left palatine bone with maxilla. (See enlarged image)
Note 43. Journal of Anatomy and Physiology, vol. xlv. The structures attached to this tubercle are: (1) the check ligament of the Rectus lateralis; (2) the lateral end of the aponeurosis of the Levator palpebræ superioris; (3) the suspensory ligament of the eye (Lockwood); and (4) the lateral extremities of the superior and inferior tarsi. [back]
You are welcome to ask for hospital review for residency. We will be providing them to those who ask them first.
The United States Medical Licensing Examination (USMLE) is a three-step examination for medical licensure in the United States. The Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME) sponsors USMLE.
The Three Steps of the USMLE
Step 1 tests the important concepts of basic sciences basic to the practice of medicine. It also places special emphasis on principles and mechanisms underlying health, disease, and modes of therapy. Step 1 ensures mastery of the sciences that provide a foundation for the safe and competent practice of medicine. It also tests the scientific principles required for maintenance of competence through lifelong learning.
Step 2 CK tests the medical knowledge, skills, and understanding of clinical science essential for the provision of patient care under supervision. It also includes emphasis on health promotion and disease prevention. Step 2 CK ensures that due attention is devoted to principles of clinical sciences and basic patient-centered skills.
Step 2 CS tests your capacity to practice and provide good medical service in real-life situations. It also tests your communication skills.
Step 3 tests your medical knowledge and understanding of biomedical and clinical science essential for the unsupervised practice of medicine. Step 3 provides a final assessment of physicians assuming independent responsibility for delivering general medical care.