|
12. Surface Markings of the Upper Extremity
|
| Bony Landmarks.—The bony landmarks as described above are so readily available for surface recognition that no special measurements are required to indicate them. It may be noted, however, that the medial angle of the scapula is applied to the second rib, while the inferior angle lies against the seventh. The intertubercular groove of the humerus is vertically below the acromioclavicular joint when the arm hangs by the side with the palm of the hand forward. | 1 |
| |
| Articulations.—The acromioclavicular joint is situated in a plane passing sagittally through the middle line of the front of the arm. The line of the elbow-joint is not straight; the radiohumeral portion is practically at right angles to the long axis of the humerus and is situated about 2 cm. distal to the lateral epicondyle; the ulnohumeral portion is oblique, and its medial end is about 2.5 cm. distal to the medial epicondyle. The position of the wrist-joint can be indicated by drawing a curved line, with its convexity upward, between the styloid processes of the radius and ulna; the summit of the convexity is about 1 cm. above the center of a straight line joining the two processes. | 2 |
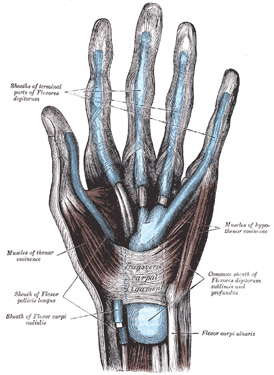 |
FIG. 1233– The mucous sheaths of the tendons on the front of the wrist and digits. (See enlarged image) |
| |
| |
| Muscles.—The only muscles of the upper extremity which occasionally require definition by surface lines are the Trapezius, the Latissimus dorsi, and the Pectorales major and minor. The antero-superior border of Trapezius is indicated by a line from the superior nuchal line about 3 cm. lateral to the external occipital protuberance to the junction of the intermediate and lateral thirds of the clavicle; the line of the lower border extends from the spinous process of the twelfth thoracic vertebra to the vertebral border of the scapula at the root of the spine. The upper border of Latissimus dorsi is almost horizontal, running from the spinous process of the seventh thoracic vertebra to the inferior angle of the scapula and thence somewhat obliquely to the intertubercular sulcus of the humerus; the lower border corresponds roughly to a line drawn from the iliac crest about 2 cm. from the lateral margin of the Sacrospinalis to the intertubercular sulcus. The upper margin of Pectoralis major extends from the middle of the clavicle to the surgical neck of the humerus; its lower border is practically in the line of the fifth rib and reaches from the fifth costochondral junction to the middle of the anterior border of Deltoideus. The two lines indicating the borders of Pectoralis minor begin at the coracoid process of the scapula and extend to the third and fifth ribs respectively, just lateral to the corresponding costal cartilages. On the front of the elbow-joint a triangular space—the anticubital fossa—is mapped out for convenience of reference. The base of the triangle is a line joining the medial and lateral epicondyles, while the sides are formed respectively by the salient margins of the Brachioradialis and Pronator teres. | 3 |
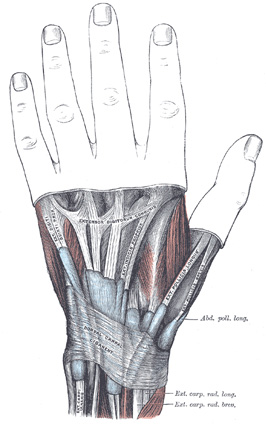 |
FIG. 1234– The mucous sheaths of the tendons on the back of the wrist. (See enlarged image) |
| |
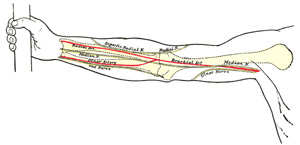 |
FIG. 1235– Front of right upper extremity, showing surface markings for bones, arteries, and nerves. (See enlarged image) |
| |
| |
| Mucous Sheaths.—On the volar surfaces of the wrist and hand the mucous sheaths of the Flexor tendons (Fig. 1233) can be indicated as follows. The sheath for Flexor pollicis longus extends from about 3 cm. above the upper edge of the transverse carpal ligament to the terminal phalanx of the thumb. The common sheath for the Flexores digitorum reaches about 3.5 to 4 cm. above the upper edge of the transverse carpal ligament and extends on the palm of the hand to about the level of the centers of the metacarpal bones. The sheath for the tendons to the little finger is continued from the common sheath to the base of the terminal phalanx of this finger; the sheaths for the tendons of the other fingers are separated from the common sheath by an interval; they begin opposite the necks of the metacarpal bones and extend to the terminal phalanges. The mucous sheaths of the Extensor tendons are shown in Fig. 1234 (see alos page 459). | 4 |
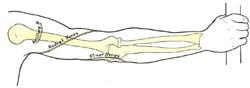 |
FIG. 1236– Back of right upper extremity, showing surface markings for bones and nerves. (See enlarged image) |
| |
| |
| Arteries (Fig. 1235).—The course of the axillary artery can be marked out by abducting the arm to a right angle and drawing a line from the middle of the clavicle to the point where the tendon of the Pectoralis major crosses the prominence of the Coracobrachialis. Of the branches of the axillary artery, the origin of the thoracoacromial corresponds to the point where the artery crosses the upper border of Pectoralis minor; the lateral thoracic takes practically the line of the lower border of Pectoralis minor; the subscapular is sufficiently indicated by the axillary border of the scapula; the scapular circumflex is given off the subscapular opposite the midpoint of a line joining the tip of the acromion to the lower edge of the deltoid tuberosity, while the humeral circumflex arteries arise from the axillary about 2 cm. above this. The position of the brachial artery is marked by a line drawn from the junction of the anterior and middle thirds of the distance between the anterior and posterior axillary folds to a point midway between the epicondyles of the humerus and continued distally for 2.5 cm., at which point the artery bifurcates. With regard to the branches of the brachial artery—the profunda crosses the back of the humerus at the level of the insertion of Deltoideus; the nutrient is given off opposite the middle of the body of the humerus; a line from this point to the back of the medial condyle represents the superior ulnar collateral; the inferior ulnar collateral is given off about 5 cm. above the fold of the elbow-joint and runs directly medialward. | 5 |
| The position of the radial artery in the forearm is represented by a line from the lateral margin of the Biceps tendon in the center of the anticubital fossa to the medial side of the front of the styloid process of the radius when the limb is in the position of supination. The situation of the distal portion of the artery is indicated by continuing this line around the radial side of the wrist to the proximal end of the first intermetacarpal space. | 6 |
| On account of the curved direction of the ulnar artery, two lines are required to indicate its course; one is drawn from the front of the medial epicondyle to the radial side of the pisiform bone; the lower two-thirds of this line represents two-thirds of the artery; the upper third is represented by a second line from the center of the hollow in front of the elbow-joint to the junction of the upper and middle thirds of the first line. | 7 |
| The superficial volar arch (Fig. 1237) can be indicated by a line starting from the radial side of the pisiform bone and curving distalward and lateralward as far as the base of the thumb, with its convexity toward the fingers. The summit of the arch is usually on a level with the ulnar border of the outstretched thumb. The deep volar arch is practically transverse, and is situated about 1 cm. nearer to the carpus. | 8 |
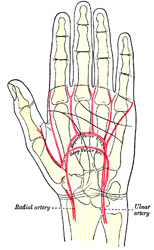 |
FIG. 1237– Palm of left hand, showing position of skin creases and bones, and surface markings for the volar arches. (See enlarged image) |
| |
| |
| Nerves (Figs. 1235, 1236).—In the arm the line of the median nerve is practically the same as that for the brachial artery; at the bend of the elbow the nerve is medial to the artery. The course of the nerve in the forearm is marked by a line starting from a point just medial to the center of one joining the epicondyles, and extending to the lateral margin of the tendon of Palmaris longus at the wrist. | 9 |
| The ulnar nerve follows the line of the brachial artery in the upper half of the arm, but at the middle of the arm it diverges and descends to the back of the medial epicondyle. In the forearm it is represented by a line from the front of the medial epicondyle to the radial side of the pisiform bone. | 10 |
| The course of the radial nerve can be indicated by a line from just below the posterior axillary fold, to the lateral side of the humerus at the junction of its middle and lower thirds; thence it passes vertically downward on the front of the arm to the level of the lateral epicondyle. The course of the superficial radial nerve is represented by a continuation of this line downward to the junction of the middle and lower thirds of the radial artery; it then crosses the radius and runs distalward to the dorsum of the base of the first metacarpal bone. | 11 |
| The axillary nerve crosses the humerus about 2 cm. above the center of a line joining the tip of the acromion to the lower edge of the deltoid tuberosity. | 12 |
