The anterior divisions of the thoracic nerves (rami anteriores; ventral divisions) are twelve in number on either side. Eleven of them are situated between the ribs, and are therefore termed intercostal; the twelfth lies below the last rib. Each nerve is connected with the adjoining ganglion of the sympathetic trunk by a gray and a white ramus communicans. The intercostal nerves are distributed chiefly to the parietes of the thorax and abdomen, and differ from the anterior divisions of the other spinal nerves, in that each pursues an independent course, i. e., there is no plexus formation. The first two nerves supply fibers to the upper limb in addition to their thoracic branches; the next four are limited in their distribution to the parietes of the thorax; the lower five supply the parietes of the thorax and abdomen. The twelfth thoracic is distributed to the abdominal wall and the skin of the buttock.
The First Thoracic Nerve.—The anterior division of the first thoracic nerve divides into two branches: one, the larger, leaves the thorax in front of the neck of the first rib, and enters the brachial plexus; the other and smaller branch, the first intercostal nerve, runs along the first intercostal space, and ends on the front of the chest as the first anterior cutaneous branch of the thorax. Occasionally this anterior cutaneous branch is wanting. The first intercostal nerve as a rule gives off no lateral cutaneous branch; but sometimes it sends a small branch to communicate with the intercostobrachial. From the second thoracic nerve it frequently receives a connecting twig, which ascends over the neck of the second rib.
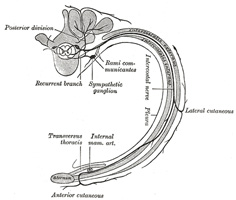
FIG. 819– Diagram of the course and branches of a typica intercostal nerve. (See enlarged image)
The Upper Thoracic Nerves (nn. intercostales).—The anterior divisions of the second, third, fourth, fifth, and sixth thoracic nerves, and the small branch from the first thoracic, are confined to the parietes of the thorax, and are named thoracic intercostal nerves. They pass forward (Fig. 819) in the intercostal spaces below the intercostal vessels. At the back of the chest they lie between the pleura and the posterior intercostal membranes, but soon pierce the latter and run between the two planes of Intercostal muscles as far as the middle of the rib. They then enter the substance of the Intercostales interni, and, running amidst their fibers as far as the costal cartilages, they gain the inner surfaces of the muscles and lie between them and the pleura. Near the sternum, they cross in front of the internal mammary artery and Transversus thoracis muscle, pierce the Intercostales interni, the anterior intercostal membranes, and Pectoralis major, and supply the integument of the front of the thorax and over the mamma, forming the anterior cutaneous branches of the thorax; the branch from the second nerve unites with the anterior supraclavicular nerves of the cervical plexus.
Branches.—Numerous slender muscular filaments supply the Intercostales, the Subcostales, the Levatores costarum, the Serratus posterior superior, and the Transversus thoracis. At the front of the thorax some of these branches cross the costal cartilages from one intercostal space to another.
Lateral cutaneous branches (rami cutanei laterales) are derived from the intercostal nerves, about midway between the vertebræ and sternum; they pierce the Intercostales externi and Serratus anterior, and divide into anterior and posterior branches. The anterior branches run forward to the side and the forepart of the chest, supplying the skin and the mamma; those of the fifth and sixth nerves supply the upper digitations of the Obliquus externus abdominis. The posterior branches run backward, and supply the skin over the scapula and Latissimus dorsi.
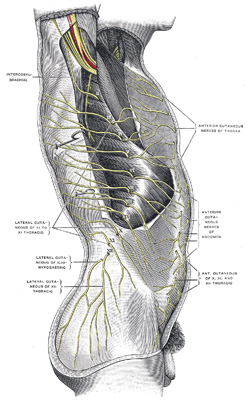
FIG. 820– Cutaneous distribution of thoracic nerves. (Testut.) (See enlarged image)
The lateral cutaneous branch of the second intercostal nerve does not divide, like the others, into an anterior and a posterior branch; it is named the intercostobrachial nerve(Fig. 816). It pierces the Intercostalis externus and the Serratus anterior, crosses the axilla to the medial side of the arm, and joins with a filament from the medial brachial cutaneous nerve. It then pierces the fascia, and supplies the skin of the upper half of the medial and posterior part of the arm, communicating with the posterior brachial cutaneous branch of the radial nerve. The size of the intercostobrachial nerve is in inverse proportion to that of the medial brachial cutaneous nerve. A second intercostobrachial nerve is frequently given off from the lateral cutaneous branch of the third intercostal; it supplies filaments to the axilla and medial side of the arm.
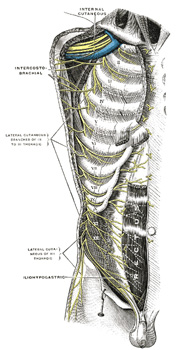
FIG. 821– Intercostal nerves, the superficial muscles having been removed. (Testut). (See enlarged image)
The Lower Thoracic Nerves.—The anterior divisions of the seventh, eighth, ninth, tenth, and eleventh thoracic nerves are continued anteriorly from the intercostal spaces into the abdominal wall; hence they are named thoracicoabdominal intercostal nerves. They have the same arrangement as the upper ones as far as the anterior ends of the intercostal spaces, where they pass behind the costal cartilages, and between the Obliquus internus and Transversus abdominis, to the sheath of the Rectus abdominis, which they perforate. They supply the Rectus abdominis and end as the anterior cutaneous branches of the abdomen; they supply the skin of the front of the abdomen. The lower intercostal nerves supply the Intercostales and abdominal muscles; the last three send branches to the Serratus posterior inferior. About the middle of their course they give off lateral cutaneous branches. These pierce the Intercostales externi and the Obliquus externus abdominis, in the same line as the lateral cutaneous branches of the upper thoracic nerves, and divide into anterior and posterior branches, which are distributed to the skin of the abdomen and back; the anterior branches supply the digitations of the Obliquus externus abdominis, and extend downward and forward nearly as far as the margin of the Rectus abdominis; the posterior branches pass backward to supply the skin over the Latissimus dorsi.
The anterior division of the twelfth thoracic nerve is larger than the others; it runs along the lower border of the twelfth rib, often gives a communicating branch to the first lumbar nerve, and passes under the lateral lumbocostal arch. It then runs in front of the Quadratus lumborum, perforates the Transversus, and passes forward between it and the Obliquus internus to be distributed in the same manner as the lower intercostal nerves. It communicates with the iliohypogastric nerve of the lumbar plexus, and gives a branch to the Pyramidalis. The lateral cutaneous branch of the last thoracic nerve is large, and does not divide into an anterior and a posterior branch. It perforates the Obliqui internus and externus, descends over the iliac crest in front of the lateral cutaneous branch of the iliohypogastric (Fig. 819), and is distributed to the skin of the front part of the gluteal region, some of its filaments extending as low as the greater trochanter.
The United States Medical Licensing Examination (USMLE) is a three-step examination for medical licensure in the United States. The Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME) sponsors USMLE.
The Three Steps of the USMLE
Step 1 tests the important concepts of basic sciences basic to the practice of medicine. It also places special emphasis on principles and mechanisms underlying health, disease, and modes of therapy. Step 1 ensures mastery of the sciences that provide a foundation for the safe and competent practice of medicine. It also tests the scientific principles required for maintenance of competence through lifelong learning.
Step 2 CK tests the medical knowledge, skills, and understanding of clinical science essential for the provision of patient care under supervision. It also includes emphasis on health promotion and disease prevention. Step 2 CK ensures that due attention is devoted to principles of clinical sciences and basic patient-centered skills.
Step 2 CS tests your capacity to practice and provide good medical service in real-life situations. It also tests your communication skills.
Step 3 tests your medical knowledge and understanding of biomedical and clinical science essential for the unsupervised practice of medicine. Step 3 provides a final assessment of physicians assuming independent responsibility for delivering general medical care.