The posterior tibial artery(Fig. 551) begins at the lower border of the Popliteus, opposite the interval between the tibia and fibula; it extends obliquely downward, and, as it descends, it approaches the tibial side of the leg, lying behind the tibia, and in the lower part of its course is situated midway between the medial malleolus and the medial process of the calcaneal tuberosity. Here it divides beneath the origin of the Adductor hallucis into the medial and lateral plantar arteries.
Relations.—The posterior tibial artery lies successively upon the Tibialis posterior, the Flexor digitorum longus, the tibia, and the back of the ankle-joint. It is covered by the deep transverse fascia of the leg, which separates it above from the Gastrocnemius and Soleus; at its termination it is covered by the Abductor hallucis. In the lower third of the leg, where it is more superficial, it is covered only by the integument and fascia, and runs parallel with the medial border of the tendo calcaneus. It is accompanied by two veins, and by the tibial nerve, which lies at first to the medial side of the artery, but soon crosses it posteriorly, and is in the greater part of its course on its lateral side.
Behind the medial malleolus, the tendons, bloodvessels, and nerve are arranged, under cover of the laciniate ligament, in the following order from the medial to the lateral side: (1) the tendons of the Tibialis posterior and Flexor digitorum longus, lying in the same groove, behind the malleolus, the former being the more medial. Next is the posterior tibial artery, with a vein on either side of it; and lateral to the vessels is the tibial nerve; about 1.25 cm. nearer the heel is the tendon of the Flexor hallucis longus.
Peculiarities in Size.—The posterior tibial is not infrequently smaller than usual, or absent, its place being supplied by a large peroneal artery, which either joins the small posterior tibial artery, or continues alone to the sole of the foot.
The peroneal artery (a. peronæa) is deeply seated on the back of the fibular side of the leg. It arises from the posterior tibial, about 2.5 cm. below the lower border of the Popliteus, passes obliquely toward the fibula, and then descends along the medial side of that bone, contained in a fibrous canal between the Tibialis posterior and the Flexor hallucis longus, or in the substance of the latter muscle. It then runs behind the tibiofibular syndesmosis and divides into lateral calcaneal branches which ramify on the lateral and posterior surfaces of the calcaneus.
Peculiarities in Origin.—The peroneal artery may arise 7 or 8 cm. below the Popliteus, or from the posterior tibial high up, or even from the popliteal.
Its size is more frequently increased than diminished; and then it either reinforces the posterior tibial by its junction with it, or altogether takes the place of the posterior tibial in the lower part of the leg and foot, the latter vessel only existing as a short muscular branch. In those rare cases where the peroneal artery is smaller than usual, a branch from the posterior tibial supplies its place; and a branch from the anterior tibial compensates for the diminished anterior peroneal artery. In one case the peroneal artery was entirely wanting.
The Perforating Branch (ramus perforans; anterior peroneal artery) pierces the interosseous membrane, about 5 cm. above the lateral malleolus, to reach the front of the leg, where it anastomoses with the anterior lateral malleolar; it then passes down in front of the tibiofibular syndesmosis, gives branches to the tarsus, and anastomoses with the lateral tarsal. The perforating branch is sometimes enlarged, and takes the place of the dorsalis pedis artery.
The Communicating Branch (ramus communicans) is given off from the peroneal about 2.5 cm. from its lower end, and joins the communicating branch of the posterior tibial.
The Lateral Calcaneal (ramus calcaneus lateralis; external calcaneal) are the terminal branches of the peroneal artery; they pass to the lateral side of the heel, and communicate with the lateral malleolar and, on the back of the heel, with the medial calcaneal arteries.
The nutrient artery (a. nutricia tibiæ) of the tibia arises from the posterior tibial, near its origin, and after supplying a few muscular branches enters the nutrient canal of the bone, which it traverses obliquely from above downward. This is the largest nutrient artery of bone in the body.
The posterior medial malleolar artery (a. malleolaris posterior medialis; internal malleolar artery) is a small branch which winds around the tibial malleolus and ends in the medial malleolar net-work.
The communicating branch (ramus communicans) runs transversely across the back of the tibia, about 5 cm. above its lower end, beneath the Flexor hallucis longus, and joins the communicating branch of the peroneal.
The medial calcaneal (rami calcanei mediales; internal calcaneal) are several large arteries which arise from the posterior tibial just before its division; they pierce the laciniate ligament and are distributed to the fat and integument behind the tendo calcaneus and about the heel, and to the muscles on the tibial side of the sole, anastomosing with the peroneal and medial malleolar and, on the back of the heel, with the lateral calcaneal arteries.
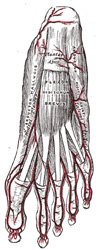
The medial plantar artery (a. plantaris medialis; internal plantar artery) (Figs. 554 and 555), much smaller than the lateral, passes forward along the medial side of the foot. It is at first situated above the Abductor hallucis, and then between it and the Flexor digitorum brevis, both of which it supplies. At the base of the first metatarsal bone, where it is much diminished in size, it passes along the medial border of the first toe, anastomosing with the first dorsal metatarsal artery. Small superficial digital branches accompany the digital branches of the medial plantar nerve and join the plantar metatarsal arteries of the first three spaces.
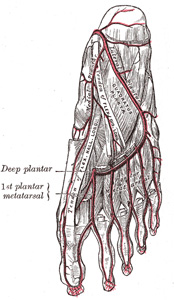
The lateral plantar artery (a. plantaris lateralis; external plantar artery), much larger than the medial, passes obliquely lateralward and forward to the base of the fifth metatarsal bone. It then turns medialward to the interval between the bases of the first and second metatarsal bones, where it unites with the deep plantar branch of the dorsalis pedis artery, thus completing the plantar arch. As this artery passes lateralward, it is first placed between the calcaneus and Abductor hallucis, and then between the Flexor digitorum brevis and Quadratus plantæ as it runs forward to the base of the little toe it lies more superficially between the Flexor digitorum brevis and Abductor digiti quinti, covered by the plantar aponeurosis and integument. The remaining portion of the vessel is deeply situated; it extends from the base of the fifth metatarsal bone to the proximal part of the first interosseous space, and forms the plantar arch; it is convex forward, lies below the bases of the second, third, and fourth metatarsal bones and the corresponding Interossei, and upon the oblique part of the Adductor hallucis.
Branches.—The plantar arch, besides distributing numerous branches to the muscles, integument, and fasciæ in the sole, gives off the following branches:
The Perforating Branches (rami perforantes) are three in number; they ascend through the proximal parts of the second, third, and fourth interosseous spaces, between the heads of the Interossei dorsales, and anastomose with the dorsal metatarsal arteries.
The Plantar Metatarsal Arteries (aa. metatarseæ plantares; digital branches) are four in number, and run forward between the metatarsal bones and in contact with the Interossei. Each divides into a pair of plantar digital arteries which supply the adjacent sides of the toes. Near their points of division each sends upward an anterior perforating branch to join the corresponding dorsal metatarsal artery. The first plantar metatarsal artery (arteria princeps hallucis) springs from the junction between the lateral plantar and deep plantar arteries and sends a digital branch to the medial side of the first toe. The digital branch for the lateral side of the fifth toe arise from the lateral plantar artery near the base of the fifth metatarsal bone.
The United States Medical Licensing Examination (USMLE) is a three-step examination for medical licensure in the United States. The Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME) sponsors USMLE.
The Three Steps of the USMLE
Step 1 tests the important concepts of basic sciences basic to the practice of medicine. It also places special emphasis on principles and mechanisms underlying health, disease, and modes of therapy. Step 1 ensures mastery of the sciences that provide a foundation for the safe and competent practice of medicine. It also tests the scientific principles required for maintenance of competence through lifelong learning.
Step 2 CK tests the medical knowledge, skills, and understanding of clinical science essential for the provision of patient care under supervision. It also includes emphasis on health promotion and disease prevention. Step 2 CK ensures that due attention is devoted to principles of clinical sciences and basic patient-centered skills.
Step 2 CS tests your capacity to practice and provide good medical service in real-life situations. It also tests your communication skills.
Step 3 tests your medical knowledge and understanding of biomedical and clinical science essential for the unsupervised practice of medicine. Step 3 provides a final assessment of physicians assuming independent responsibility for delivering general medical care.