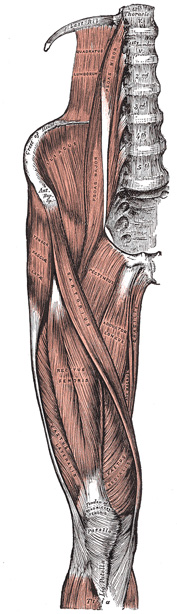
FIG. 430– Muscles of the iliac and anterior femoral regions. (See enlarged image)
The portion covering the Psoas is thickened above to form the medial lumbocostal arch, which stretches from the transverse process of the first lumbar vertebra to the body of the second. Medially, it is attached by a series of arched processes to the intervertebral fibrocartilages, and prominent margins of the bodies of the vertebræ, and to the upper part of the sacrum; the intervals left, opposite the constricted portions of the bodies, transmit the lumbar arteries and veins and filaments of the sympathetic trunk. Laterally, above the crest of the ilium, it is continuous with the fascia covering the front of the Quadratus lumborum (see page 419), while below the crest of the ilium it is continuous with the fascia covering the Iliacus.
The portions investing the Iliacus (fascia iliaca; iliac fascia) is connected, laterally to the whole length of the inner lip of the iliac crest; and medially, to the linea terminalis of the lesser pelvis, where it is continuous with the periosteum. At the iliopectineal eminence it receives the tendon of insertion of the Psoas minor, when that muscle exists. Lateral to the femoral vessels it is intimately connected to the posterior margin of the inguinal ligament, and is continuous with the transversalis fascia. Immediately lateral to the femoral vessels the iliac fascia is prolonged backward and medialward from the inguinal ligament as a band, the iliopectineal fascia, which is attached to the iliopectineal eminence. This fascia divides the space between the inguinal ligament and the hip bone into two lacunæ or compartments, the medial of which transmits the femoral vessels, the lateral the Psoas major and Iliacus and the femoral nerve. Medial to the vessels the iliac fascia is attached to the pectineal line behind the inguinal aponeurotic falx, where it is again continuous with the transversalis fascia. On the thigh the fasciæ of the Iliacus and Psoas form a single sheet termed the iliopectineal fascia. Where the external iliac vessels pass into the thigh, the fascia descends behind them, forming the posterior wall of the femoral sheath. The portion of the iliopectineal fascia which passes behind the femoral vessels is also attached to the pectineal line beyond the limits of the attachment of the inguinal aponeurotic falx; at this part it is continuous with the pectineal fascia. The external iliac vessels lie in front of the iliac fascia, but all the branches of the lumbar plexus are behind it; it is separated from the peritoneum by a quantity of loose areolar tissue.
The Psoas major (Psoas magnus) (Fig. 430) is a long fusiform muscle placed on the side of the lumbar region of the vertebral column and brim of the lesser pelvis. It arises (1) from the anterior surfaces of the bases and lower borders of the transverse processes of all the lumbar vertebræ (2) from the sides of the bodies and the corresponding intervertebral fibrocartilages of the last thoracic and all the lumbar vertebræ by five slips, each of which is attached to the adjacent upper and lower margins of two vertebræ, and to the intervertebral fibrocartilage; (3) from a series of tendinous arches which extend across the constricted parts of the bodies of the lumbar vertebræ between the previous slips; the lumbar arteries and veins, and filaments from the sympathetic trunk pass beneath these tendinous arches. The muscle proceeds downward across the brim of the lesser pelvis, and diminishing gradually in size, passes beneath the inguinal ligament and in front of the capsule of the hip-joint and ends in a tendon; the tendon receives nearly the whole of the fibers of the Iliacus and is inserted into the lesser trochanter of the femur. A large bursa which may communicate with the cavity of the hip-joint, separates the tendon from the pubis and the capsule of the joint.
The Psoas minor (Psoas parvus) is a long slender muscle, placed in front of the Psoas major. It arises from the sides of the bodies of the twelfth thoracic and first lumbar vertebræ and from the fibrocartilage between them. It ends in a long flat tendon which is inserted into the pectineal line and iliopectineal eminence, and, by its lateral border, into the iliac fascia. This muscle is often absent.
The Iliacus is a flat, triangular muscle, which fills the iliac fossa. It arises from the upper two-thirds of this fossa, and from the inner lip of the iliac crest; behind, from the anterior sacroiliac and the iliolumbar ligaments, and base of the sacrum; in front, it reaches as far as the anterior superior and anterior inferior iliac spines, and the notch between them. The fibers converge to be inserted into the lateral side of the tendon of the Psoas major, some of them being prolonged on to the body of the femur for about 2.5 cm. below and in front of the lesser trochanter.85
Variations.—The Iliacus minor or Iliocapsularis, a small detached part of the Iliacus is frequently present. It arises from the anterior inferior spine of the ilium and is inserted into the lower part of the intertrochanteric line of the femur or into the iliofemoral ligament.
Nerves.—The Psoas major is supplied by branches of the second and third lumbar nerve; the Psoas minor by a branch of the first lumbar nerve; and the Iliacus by branches of the second and third lumbar nerves through the femoral nerve.
Actions.—The Psoas major, acting from above, flexes the thigh upon the pelvis, being assisted by the Iliacus; acting from below, with the femur fixed, it bends the lumbar portion of the vertebral column forward and to its own side, and then, in conjunction with the Iliacus, tilts the pelvis forward. When the muscles of both sides are acting from below, they serve to maintain the erect posture by supporting the vertebral column and pelvis upon the femora, or in continued action bend the trunk and pelvis forward, as in raising the trunk from the recumbent posture.
The United States Medical Licensing Examination (USMLE) is a three-step examination for medical licensure in the United States. The Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME) sponsors USMLE.
The Three Steps of the USMLE
Step 1 tests the important concepts of basic sciences basic to the practice of medicine. It also places special emphasis on principles and mechanisms underlying health, disease, and modes of therapy. Step 1 ensures mastery of the sciences that provide a foundation for the safe and competent practice of medicine. It also tests the scientific principles required for maintenance of competence through lifelong learning.
Step 2 CK tests the medical knowledge, skills, and understanding of clinical science essential for the provision of patient care under supervision. It also includes emphasis on health promotion and disease prevention. Step 2 CK ensures that due attention is devoted to principles of clinical sciences and basic patient-centered skills.
Step 2 CS tests your capacity to practice and provide good medical service in real-life situations. It also tests your communication skills.
Step 3 tests your medical knowledge and understanding of biomedical and clinical science essential for the unsupervised practice of medicine. Step 3 provides a final assessment of physicians assuming independent responsibility for delivering general medical care.